Knee replacement (knee endoprosthesis) is a successful operation for many patients with advanced wear and tear of the knee joint. However, around 15 % of patients are not completely satisfied or even dissatisfied with the result. There are many reasons for this, including infection, bone fracture or instability, which can lead to permanent complaints. However, it is often the case that none of the specified causes can be identified as the cause of symptoms in patients with permanent complaints after knee replacement, and in addition, the X-ray shows no abnormalities and a straight leg.
HOW DOES THE CONVENTIONAL INSTALLATION OF A KNEE PROSTHESIS WORK?
With conventional knee arthroplasty, the aim is for every patient to have a straight leg after the operation – regardless of whether they previously had a bow leg or knock-knee. This means that all knees are operated on according to the same procedure regardless of individual differences (Figures A and B).
However, people with a completely straight leg and a perpendicular joint line are rare; the majority have a more or less pronounced bow leg or knock-knee.
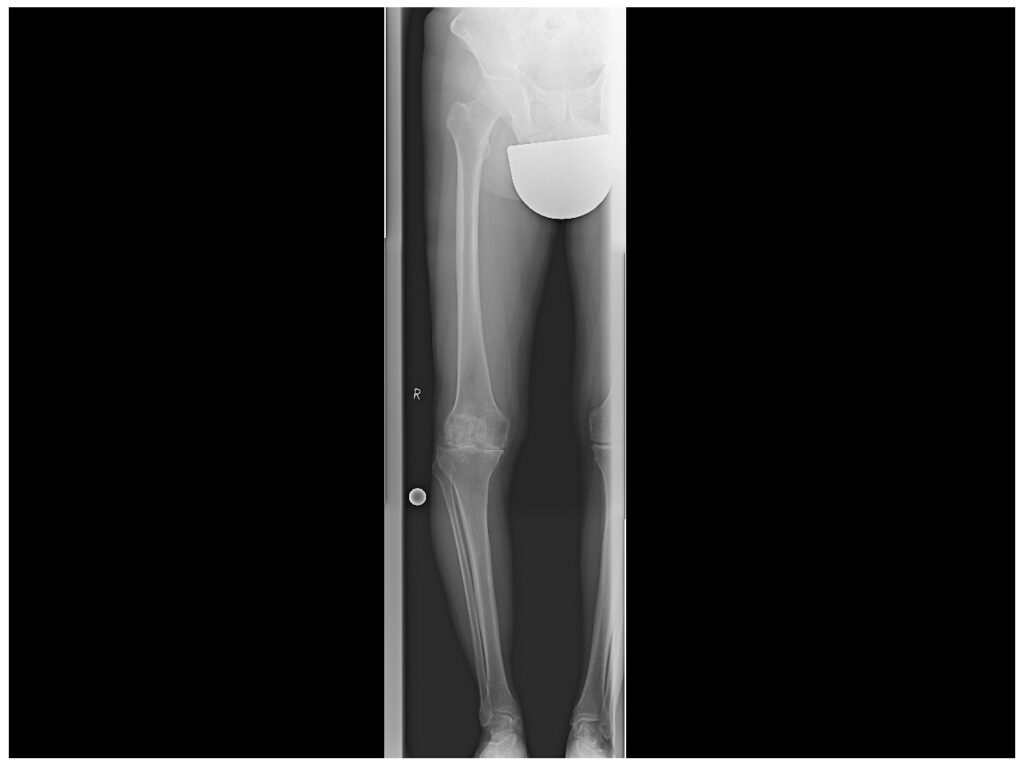
X-ray of the entire right leg
This patient has osteoarthritis of the knee: the joint space between the femur and tibia (blue arrow) is no longer present on the medial side. The red line connecting the centre of the hip and the knee or the centre of the knee and the ankle (red lines) is not straight, as this patient has a bow leg.
In addition, the joint line between the upper and lower leg bones is not strictly perpendicular to the leg axis even in a healthy knee, but usually slopes slightly inwards (Figure C). This is due to the fact that people tend to walk with a narrow stance rather than a wide-legged stance for better weight distribution. Most people manage well in this position throughout their lives.
WHAT CAN BE THE CONSEQUENCES OF CONVENTIONAL INSTALLATION?
By straightening the leg and changing the joint line with the conventional implantation technique of a knee endoprosthesis, the previous anatomy of the knee joint is largely ignored. This change in the geometry of the knee joint can lead to forced guidance of the knee joint with unnatural ligament tension, poor mobility and pain.
However, the knee joint in particular is a very complex joint that reacts sensitively to changes in shape. Even minor changes to the joint line and leg axis can severely disrupt the movement sequence between the thigh and lower leg and, in particular, have a negative impact on the sliding of the kneecap. In our opinion and experience, it is therefore essential that the natural anatomy of the patient is taken into account when replacing the knee joint, as with the hip joint, and that the same implant position is not sought for all patients.
WHAT DOES KINEMATIC ALIGNMENT MEAN?
Over 15 years ago, a technique was developed in the USA with the aim of reconstructing the knee joint anatomy individually as it was before the osteoarthritis. This technique is called “kinematic alignment”.
In kinematic alignment, the knee endoprosthesis is fitted to each patient individually according to their natural anatomy in order to restore healthy knee joint movement. For example, if a patient had a bow leg (which usually increases due to wear-related cartilage loss as part of osteoarthritis), the knee is reconstructed with a mild bow position as part of the operation. More severe misalignments are of course corrected! This setting of the knee prosthesis is not only selected in extension, but over the entire course of movement. This also restores the natural tension of the ligaments over the entire range of motion, just as the patient has been used to throughout their life. This leads to a very stable and harmonious movement sequence of the knee joint without instabilities or strains. In contrast to conventional alignment, the ligaments are not lengthened during the operation but retain their original tension (Figures C and D).
WHAT ARE THE BENEFITS OF KINEMATIC ALIGNMENT FOR THE PATIENT?
With the kinematic alignment of the knee endoprosthesis, it has been shown in several high-quality scientific studies that the proportion of patients with permanent complaints can be significantly reduced. In particular, patients are more likely to have a so-called “forgotten artificial knee joint”, i.e. they can use their knee joint in everyday life like their natural knee joint and do not think about the fact that they are wearing an artificial joint. By protecting the ligaments and muscles, patients can usually be mobilised more quickly during kinematic alignment. Furthermore, biomechanical studies have confirmed that alignment using kinematic alignment also reduces joint pressure and thus the load on the implant.
In summary, with kinematic alignment, the artificial knee joint is inserted individually according to the patient’s natural anatomy, which leads to faster mobilisation and better results.
At ECOM, we have been implanting knee prostheses after kinematic alignment with great success for years. Our positive experience with this modern surgical technique is consistent with the good results of clinical studies. Last but not least, our patients benefit from a faster recovery, less surgical trauma and a knee replacement that feels more natural in many cases.
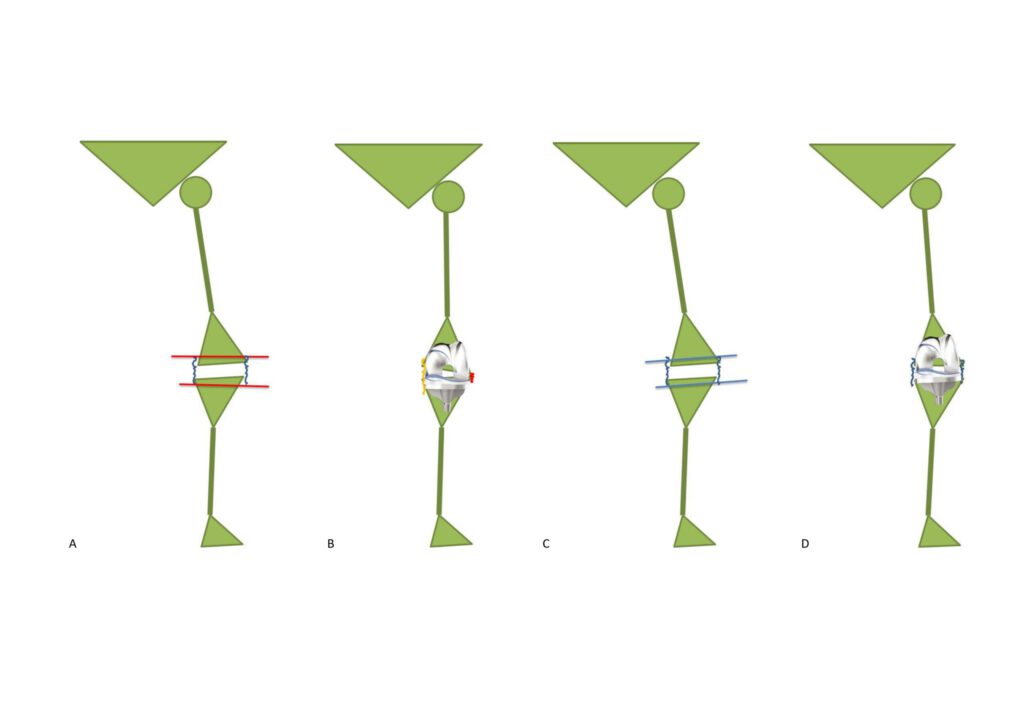
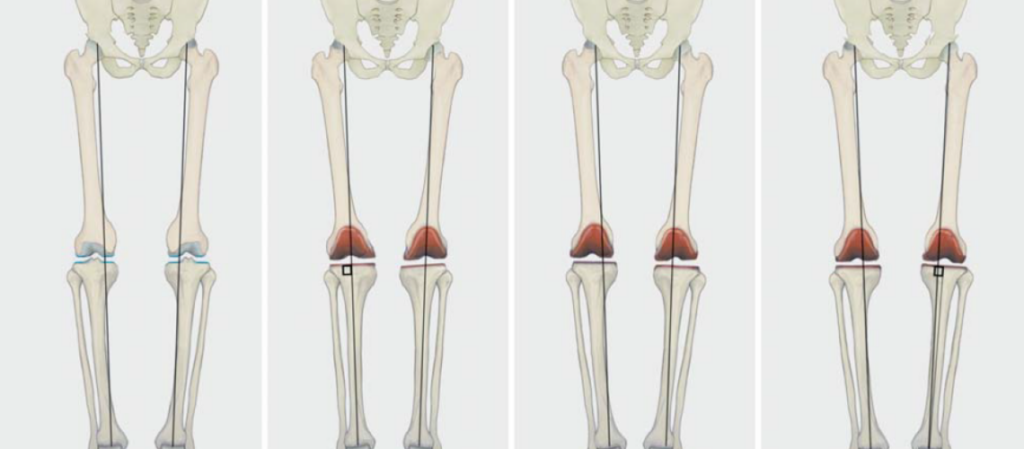
Fig. A: Schematic representation of a left leg: A slight bow leg is shown, as is often the case. The ligaments are shown in blue. The joint line slopes slightly towards the inside. The cutting planes for the conventionally inserted prosthesis are shown in red, which are not symmetrical.
Fig. B: Each leg is straightened when the prosthesis is fitted conventionally. The joint line is also set perpendicular to the leg axis regardless of the individual anatomy. In the example, this leads to overstretching of the inner ligament (in yellow) and a loose outer ligament (in orange). The inner ligament must then be surgically stretched to correct the ligament tension.
Fig. C: In kinematic alignment, the cuts for the prosthesis are customised parallel to the patient’s joint line. Taking wear into account, exactly as much of the surface is removed as is replaced by the implant. This is therefore a genuine surface replacement.
Fig. D: The knee prosthesis is inserted according to the patient’s natural anatomy. As a result, the joint line remains slightly sloping inwards. The geometry of the leg remains anatomical, with a mild bow leg. And the ligament tension remains identical to what it was naturally.
Die Mako-Roboter-Technik unterstützt den Operateur durch die Zusammenführung von 3-dimensionalen Knochen-CT-Daten einer intraoperativ erfassten Weichteilspannung und...
Sie verlassen nun den Internetauftritt der ECOM® – Praxis für Orthopädie, Sportmedizin und Unfallchirurgie Dr. Erich Rembeck, Dr. Alexander Rauch, Prof. Dr. Hans Gollwitzer, Prof. Dr. Patrick Weber – Ärztepartnerschaft aus München.
Sie werden weitergeleitet auf den Internetauftritt von ECOM – Zentrum für Regenerative Medizin und Stammzelltherapie Dr. Erich Rembeck, Dr. Alexander Rauch, Prof. Dr. Hans Gollwitzer, Prof. Dr. Patrick Weber in Thiersee, Österreich.
Die im folgenden beschriebenen Therapien finden ausschließlich in Österreich statt und sind von der Ärztekammer Tirol, sowie der Österreichische Agentur für Gesundheit und Ernährungssicherheit (AGES) genehmigt.
Bitte bestätigen Sie mit OK. Wir bedanken uns für Ihr Interesse!










")